

Androniki A. Krystalli1 DVM, Nikitas N. Prassinos1 DVM, PhD, Aikaterini I. Sideri2 DVM, PhD
1 Companion Animal Clinic, School of Veterinary Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece
2 Surgery Clinic, School of Veterinary Medicine, University of Thessaly, Karditsa, Greece
MeSH keywords:
cat, dog, femoral head, femoral neck
Abstract
Femoral head and neck excision is a salvage surgical procedure performed in both dogs and cats. During this procedure the entire femoral head and part of the femoral neck are removed at an angle starting proximal to the greater trochanter and following a direction towards the central ridge of the lesser trochanter. This procedure is intended to alleviate pain in the coxofemoral joint, which is obtained through eliminating the abnormal friction of the articular surfaces and replacing the coxofemoral joint with a functional pseudarthrosis comprised of dense fibrous connective tissue. Remodelling of the acetabulum and the proximal part of the femoral shaft may continue for several years after the procedure.
Introduction
Femoral head and neck excision (FHNE) is a salvage surgical procedure (Prostredny 2014), in which the entire femoral head and part of the femoral neck are removed at an angle, starting at the medial aspect of the greater trochanter and ending at the proximal aspect of the lesser trochanter (Schulz & Dejardin 2003). It is intended to eliminate bone-to-bone contact between the femur and acetabulum. This procedure can be performed in order to manage various coxofemoral disorders, ensuring adequate and painless coxofemoral joint function in both dogs and cats. This is obtained through elimination of the abnormal friction between articular surfaces of the coxofemoral joint and replacement of the joint by a functional pseudarthrosis which is comprised of dense fibrous connective tissue (Lewis et al., 1988, Schulz 2012, Prostredny 2014). The remodelling of the acetabulum and central part of the femur may continue for many years after the procedure (Duff & Campbell 1978).
FΗNE is recommended in the following disorders: 1) hip dysplasia, 2) avascular necrosis of the femoral head (Legg-Calvé-Perthe’s disease), 3) femoral head and/or neck fractures, 4) epiphyseolysis of the femoral head, 5) acetabular and/or pelvic fractures (usually combined with extensive soft tissue trauma), 6) chronic coxofemoral luxation or coxofemoral luxation that cannot be manually repositioned, 7) severe coxofemoral osteoarthritis with clinical implications, and 8) failed total coxofemoral arthroplasty (Berzon et al. 1980, Schulz & Dejardin 2003).
Historical review
The first to describe the FHNE technique in humans was Girdlestone, with the intention of alleviating pain in coxofemoral joint tuberculosis (Girdlestone 1928) and coxofemoral septic arthritis (Girdlestone 1943). In the following years, this technique was modified and extensively used in dogs and cats by veterinary surgeons (Ormrod 1961, Spruell 1961, Rex 1963). The results were regarded as beneficial for the management of various coxofemoral disorders (Hofmeyr 1966), such as avascular necrosis of the femoral head in dogs (Ljunggren 1967, Lee & Fry 1969). In fact, Seer & Hurov (1968) reported satisfying results even in dogs that underwent bilateral FHNE. The standard FHNE procedure remained unchanged until 1960, at which time the first total coxofemoral arthroplasty procedure was performed in humans (Charnley 1970), which was in turn modified by veterinarians and some years later it was employed in companion animals as well (Dueland 1975, Coster et al. 1981, Olmstead et al. 1983).
Surgical procedure
Preparation
In order to perform FHNE the patient is positioned in lateral recumbency with the affected limb uppermost. Clipping and surgical site aseptic preparation on the affected limb are focussed on the greater trochanter and extend to midway along the tibia. Τhe body of the patient is covered with sterilised surgical drapes, leaving the affected limb exposed, which is draped separately (e.g. with a sterilised sheath), so that manipulations during the procedure can be facilitated (Figure 1).

Figure 1. Wrapping the affected limb of a dog with sterilised
drapes during preparation for FHNE (left lateral recumbency).
Surgical site approach
The craniolateral approach to the coxofemoral joint is preferred (Denny & Butterworth 2000, Johnson & Hulse 2001, DeCamp et al. 2016), because in contrast to the dorsal approach, during the craniolateral approach the support of the femur by the gluteal muscles is preserved, the risk of causing iatrogenic fracture to the femoral diaphysis is reduced (Wallace & Olmstead 1995, Denny & Butterworth 2000) and the incisions follow the natural direction of muscle fibres (Berzon et al. 1980).
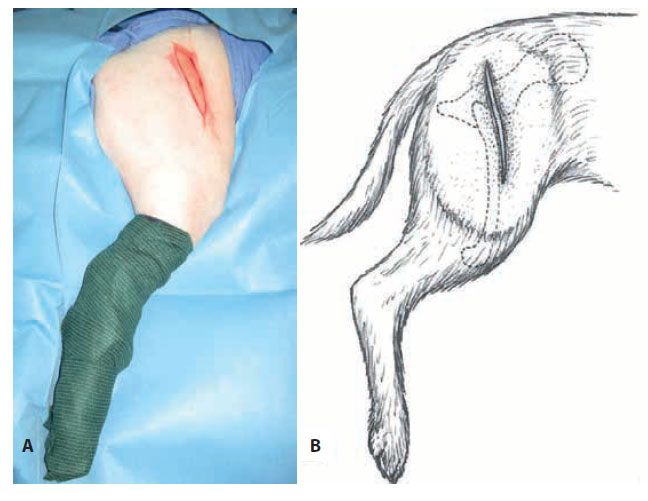
Figure 2. Initial skin incision in a dog (Α) and in schematic drawing (B - modified from Johnson [2014a]).
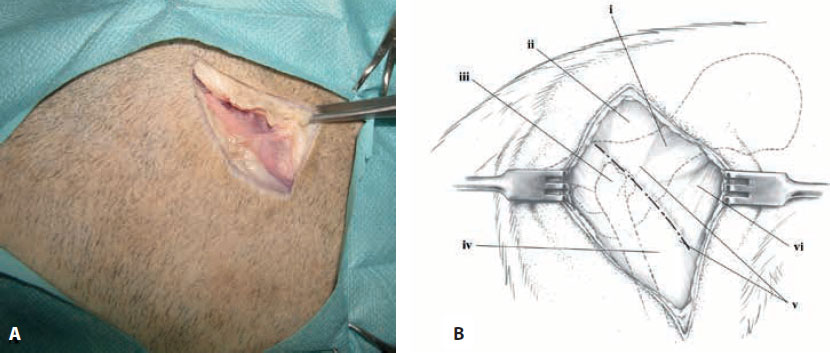
Figure 3. Incision in the superficial leaf of the fascia lata, at the cranial border of the biceps femoris muscle in a dog (Α) and in schematic drawing (Β - modified from Johnson [2014a]). i: middle gluteal muscle, ii: superficial gluteal muscle, iii: great trochanter, iv: biceps femoris muscle, v: incision in superficial leaf of fascia lata, vi: tensor fascia lata muscle.
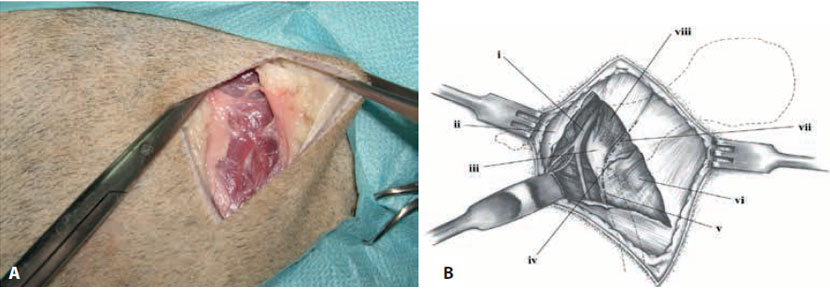
Figure 4. Incision between the deep leaf of the fascia lata and the tensor fascia lata muscle, as well as between the tensor fascia lata and thesuperficial gluteus muscle in a dog (Α) and in schematic drawing (Β - modified from Johnson [2014a]). i: sciatic nerve and caudal gluteal vein and artery, ii: biceps femoris muscle, iii: great trochanter, iv: lateral circumflex femoral artery and vein, v: incision in deep leaf of fascia lata, vi: tensor fascia lata muscle, vii: intermuscular incision, superficial gluteal muscle.
A skin incision is made initially, which begins dorsal and cranial to the greater trochanter and up to the proximal-to-median third of the femoral diaphysis (Figure 2). The subcutaneous tissues are separated from the underlying muscle and the superficial leaf of the fascia lata is incised at the cranial border of the biceps femoris muscle (Figure 3). The biceps femoris is then caudally retracted and an incision is made between the deep leaf of the fascia lata and the tensor fascia lata muscle, as well as between the tensor fascia lata muscle and the superficial gluteal muscle (Figure 4). The deep leaf of the fascia lata is retracted cranially and the biceps femoris muscle is retracted caudally. Surgical preparation and exposure of the anatomical triangle is then performed, the sides of which are comprised of the middle gluteus, the deep gluteus, the rectus femoris and the vastus lateralis muscles, in the centre of which the acetabulum can be visualised (Figure 5). In order to facilitate locating the femoral head, the greater trochanter is grasped by double-pointed (large patients) or single-pointed (smaller patients) bone reduction forceps, and by performing rotational motions the femoral head can either be visualised (large animals) and/ or palpated (smaller animals) (Figure 6). At this point special care must be taken to avoid injury of the sciatic nerve with the forceps, which runs caudal to the coxofemoral joint and over the superficial gluteal and gemelli muscles. Surgical approach to the coxofemoral joint is completed by retraction of the muscles forming the anatomical triangle with the aid of two self-retaining Gelpi retractors (Johnson 2014a), which ensure adequate exposure of the surgical site (Figure 7). In cats, during this approach, a wider incision is required at the insertion of the tendon of tensor fascia lata and wider subperiosteal elevation of the vastus lateralis muscle as well, in order to obtain sufficient exposure of the femoral neck due to the fact that the tensor fascia lata muscle and the vastus lateralis are wider in cats compared to dogs (Ablin & Gambardella 1991). Also in cats, the gluteal muscles are larger, therefore posing a challenge during exposure of the coxofemoral joint compared to dogs (Johnson 2014b).
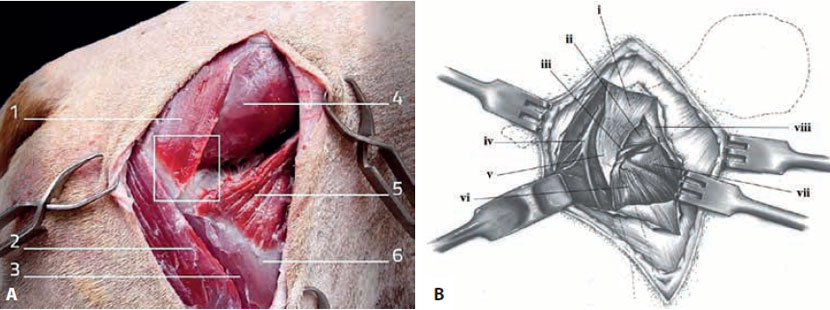
Figure 5. Exposure of the anatomical triangle formed by the superficial gluteus, the middle gluteus, the rectus femoris and the vastus lateralis
muscles in a dog. 1. Superficial gluteal muscle, 2. Biceps femoris muscle, 3. Vastus lateralis muscle, 4. Middle gluteal muscle, 5.Tensor fascia lata
muscle, 6. Fascia lata i: superficial gluteal muscle, ii: middle gluteal muscle, iii: deep gluteal muscle, iv: sciatic nerve and caudal gluteal vein and
artery, v: great trochanter, vi: vastus lateralis muscle, vii: rectus femoris muscle, viii: tensor fascia lata muscle. (Α - modified from Climent et al. [2014])
and in schematic drawing (Β - modified by Johnson [2014a]).
 Figure 6. Grasping the greater trochanter with pointed bone reduction forceps. |
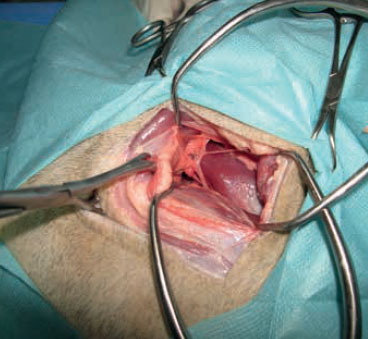 Figure 7. Placement of Gelpi retractors. |
Afterward, capsulotomy of the coxofemoral joint is performed, in cases when the joint capsule is still intact, as well as tenotomy of part of the inserting tendon of the vastus lateralis muscle if necessary (Figure 8). Capsulotomy results in the outflow of joint fluid. If necessary, partial tenotomy at the insertion of the deep gluteus muscle can also be performed (Johnson 2014a). For the luxation of the femoral head from the acetabulum, resection of the round ligament is necessary, if it remains intact, with curved Mayo scissors or special bifurcated syndesmotome (Figure 9) and then the articular capsule is detached from its insertion points to the femoral neck.
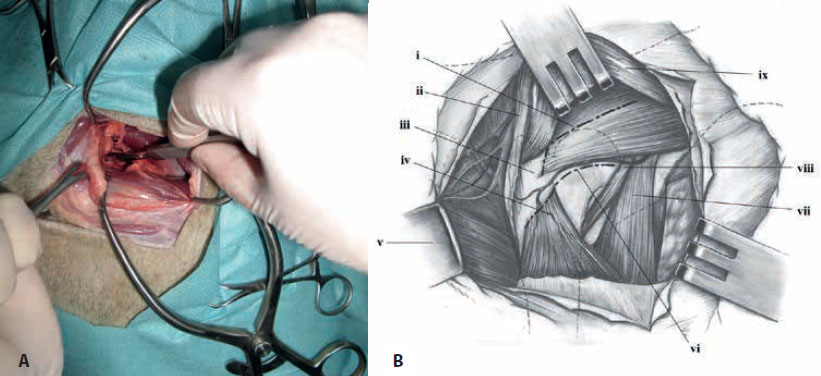
Figure 8. Capsulotomy of the coxofemoral joint and part of the insertion of the vastus lateralis muscle in a dog (Α) and in schematic drawing (Β - modified from Johnson [2014a]). i: incision in deep gluteal muscle, ii: superficial gluteal muscle, iii: great trochanter, iv: incision in origin of vastus lateralis muscle, v: biceps femoris muscle retracted, vi: incision in joint capsule, vii: rectus femoris muscle, viii: articularis coxae muscle, ix: middle gluteal muscle
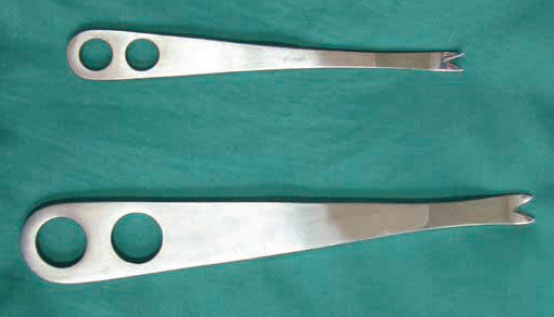
Figure 9. Small and large syndesmotome.
Τhe FHNE technique
For the ostectomy, an osteotome and hammer can be used, or an oscillating saw or a Gigli bone saw (Figure 10) (Johnson & Hulse 2001, Schulz & Dejardin 2003, DeCamp et al. 2016). Τhe width of the osteotome should correspond to the diameter of the femoral neck, e.g. for a large dog it should be at least 2.5 cm, otherwise the excision will have to occur gradually (DeCamp et al. 2016). Alternatively, in smaller dogs and cats a Rongeur osteotome can be used (Figure 11) (Schulz & Dejardin 2003). In cases of osteoporosis the osteotome and hammer should be avoided, because it may result in fracture of the greater trochanter and/or the femoral diaphysis (Berzon et al. 1980).

Figure 10. Α: Osteotome and hammer, Β: electric oscillating saw, and C: Gigli bone saw.

In order to perform the excision, the femur is laterally rotated by 90° (Johnson & Hulse 2001, Schulz & Dejardin 2003, DeCamp et al. 2016). The femoral neck is usually supported by two Ηοhman retractors (Figure 12) or curved scissors which are placed on both sides at right angles to the direction of the femoral neck (Figure 13). The line followed during the excision starts from the base of the greater trochanter proximally and extends at an angle, ending distally at the point where the femoral head is unified with the femoral diaphysis (Figure 14). Sometimes, the excision may include part of the lesser trochanter, but it is best that this is limited or avoided entirely. The direction of placement of the tool that will be used during FHNE should be parallel to the sagittal plane of the femur, because if it occurs vertically to the femoral neck, then bone fragments will remain in the caudal portion of the femoral neck (DeCamp et al. 2016).
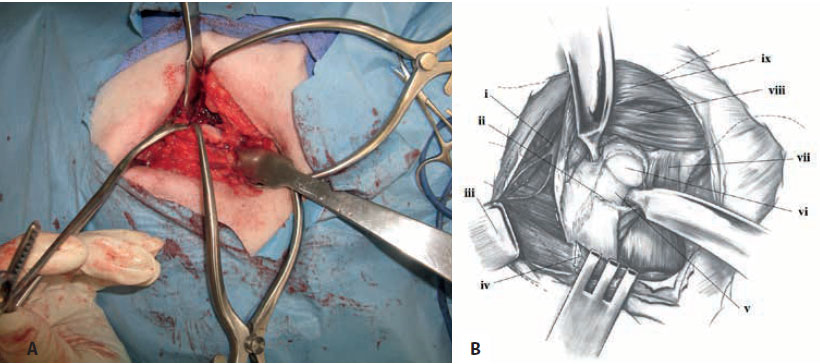
Figure 13. The Hohman retractor is inserted to support each side of the incision and at right angles to the long axis of the femoral neck in a dog (Α) and in schematic drawing (Β - modified from Johnson [2014a]). i: sciatic nerve and caudal gluteal vein and artery, ii: joint capsule, iii: biceps femoris muscle retracted, iv: vastus lateralis muscle retracted, v: femoral neck, vi: femoral head, vii: rectus femoris muscle, viii: deep gluteal muscle, ix: middle gluteal muscle.
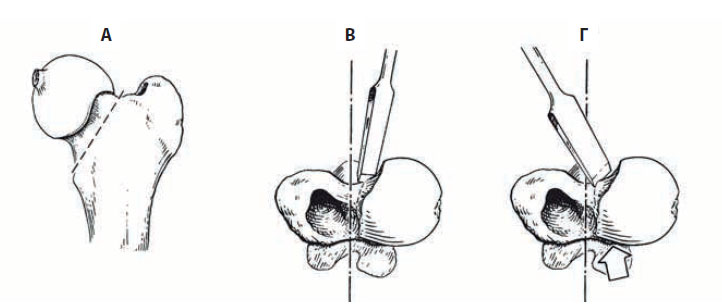
Figure 14. The direction followed during resection of the femoral head and neck. Α: lateral, Β: dorsoventral - correct, C: dorsoventral – incorrect (modified from DeCamp et al. [2016]).
Once the ostectomy is completed, the surface of the femoral neck is palpated and in case the angle of excision was incorrect or there are bone fragments, it is smoothed with an orthopaedic rasp (Figure 15), a Rongeur osteotome and/or an oscillating bone saw (Schulz & Dejardin 2003, DeCamp et al. 2016). The absence of crepitus during passive range flexion and extension motions of the coxofemoral joint indicates sufficient smoothing of the ostectomy surface (DeCamp et al. 2016). Surgical site is closed by suturing the vastus lateralis, the deep gluteus muscle in cases of tenotomy, the tensor fascia lata muscle, the subcutaneous tissue and the skin in a routine fashion (Johnson & Hulse 2001).

Figure 15. Small and large orthopaedic rasp.
Several studies have been made in order to improve the technique described above. To this purpose, surgical insertion of soft tissues such as fat or muscle between the pelvic bones and the ostectomy surface has been suggested. Partial or total transposition of a muscle has been commonly reported (Wallace & Olmstead 1995, Johnson & Hulse 2001, Schulz & Dejardin 2003), and usually the biceps femoris muscle is implicated (Mann et al. 1987, Lewis et al. 1988, Prostredny et al. 1991) or the cranial third of the deep gluteus muscle (Berzon et al. 1980). In other studies, suturing of the joint capsule is recommended (Johnson & Hulse 2001, Schulz & Dejardin 2003, Off & Matis 2010). In both cases the aim is to avoid bone contact, and therefore to offer pain relief. However, these techniques did not seem to offer any advantage compared to the standard FHNE and they are no longer recommended for routine use in the clinical setting (Roush 2012). However, the exception described by DeCamp et al. (2016) is of particular interest, regarding the transposition of the deep gluteal muscle during FHNE in cases of comminuted acetabular fractures which cannot be repaired by routine osteosynthesis. In such cases suturing the joint capsule is also recommended if feasible. Finally, wedge ostectomy has also been recommended (WRT-wedge resection technique), during which osteotomy of the greater trochanter is followed by resection of the femoral head, neck, and part of the metaphysis of the femoral shaft and finally internal fixation of the greater trochanter to the femoral metaphysis by cross pins (Figure16). However, a comparative study has shown that there is no clinical difference between this technique and routine FHNE (Montgomery et al. 1987).
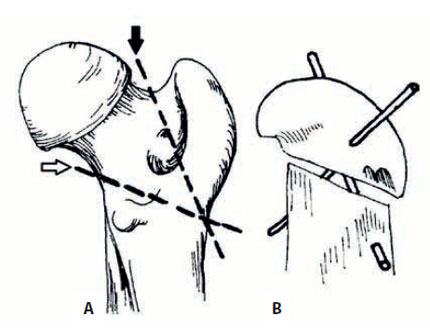
Figure 16. Femoral head wedge resection technique. Α:Greater trochanter osteotomy (black arrow), ostectomy of the femoral head, neck and part of the femoral metaphysis (white arrow). Β: Osteosynthesis of the greater trochanter to the femoral metaphysis by cross pins (modified from Montgomery [1987]).
Factors affecting the FHNE technique
In general, factors that may lead to rapid weight-bearing recovery of the limb also contribute to return to optimal function (Roush 2012).
Preoperative factors
Preoperative factors that may affect the result of FHNE include body weight, age of the patient and the chronicity of the condition that led to the procedure.
Several authors suggest that the results of FHNE are better in cats and small breed dogs (less than 17-22 kg) in comparison to large breeds (Duff & Campbell 1977, Lewis et al. 1988, Mann et al. 1993, Remedios & Fries 1995, Johnson & Hulse 2001, Schulz & Dejardin 2003, Prostredny 2014). In contrast, others suggest that FHNE is equally effective in large breed dogs, even in cases of bilateral FHNE. In truth, studies to this effect have shown that the increased body weight does not negatively affect the clinical course of such cases (Berzon et al. 1980, Rawson et al. 2005). Nevertheless, it has been generally accepted that a lot of animals that undergo FHNE do not have a normal gait postoperatively, a fact which is more obvious in large breed dogs, though whether this reflects chronic pain remains unclear. It occurs possibly due to a greater dorsal dislocation of the proximal part of the femoral bone during weight bearing, which appears to be in proportion to the body weight of the animal (Wallace & Olmstead 1995, Plante et al. 1997, Roush 2012). The affected joint that underwent surgery is also “weaker”, as proven by reduced width of the quadriceps femoris muscle in at least 50% of patients (Duff & Campbell 1977), intermittent lameness after intense exercise, and by a reduced ability to jump, which is more common in large breed dogs. All of the aforementioned observations are confirmed by motion and force plate analysis, which indicates severely reduced maximum forward force in the hindlimbs of dogs that underwent FHNE (Plante et al. 1997). Nevertheless, regardless of the above, no statistically significant results have been published connecting the percentage of successful FHNE with the body weight of the animal (Berzon et al. 1980, Manley 1993, Wallace & Olmstead 1995, DeCamp et al. 2016). Off and Matis (2010) studied motion and force plate analysis on a small number of patients that underwent FHNE and noted partial loss of function on the affected limb, not only in large but also in small patients; however in the latter case it was not so easily noticed with the naked eye due to the faster pace.
According to some authors, patient age affects the postoperative result of cases that underwent FHNE, considering that prognosis is better in young animals (Wallace & Olmstead 1995, Schulz & Dejardin 2003, Harasen 2004).
Regarding the chronicity of the disorder that led to FHNE being performed, it is reported that longer duration negatively affects postoperative outcome (Wallace & Olmstead 1995, Johnson & Hulse 2001, Schulz & Dejardin 2003). Patients with recent trauma, such as fractures of the femoral head or neck, regain affected limb function faster compared to animals with chronic disorders, such as hip dysplasia. This is attributed to muscle atrophy as well as secondary osteoarthritis lesions that develop over time (Denny & Butterworth 2000). Perhaps the loss of function of the affected limb that underwent surgery in the cases of Off and Matis (2010) that were mentioned previously can be attributed to the fact that all of the patients were affected by chronic conditions.
Intraoperative factors
Intraoperatively, the protocol followed during the surgery is of the utmost importance (Lee & Fry 1969, Wallace & Olmstead 1995, Denny & Butterworth 2000, Harasen 2004). Atraumatic surgical approach plays an important role, so that the muscles do not sustain damage that may cause a disruption in blood perfusion, as well as a loss of supportive function, which is necessary in order to prevent the dorsal transportation of the femur after FHNE (Harasen 2004). Great care should also be given to avoid damaging the large blood vessels of the area, e.g. circumflex femoral artery. Finally, an incorrect ostectomy angle, and an irregular femoral neck ostectomy surface reduce the possibility of a satisfactory postoperative outcome (Berzon et al. 1980). In contrast, the adequate excision of the femoral neck at a correct angle, as well as a smooth osteotomy surface allow the immediate and painless contact of bone surfaces (Berzon et al. 1980, Wallace & Olmstead 1995, Piek et al. 1996, DeCamp et al. 2016) and therefore a faster return to limb function.
Postoperative factors
Postoperatively, the use of analgesics, controlled physical activity and physiotherapy are factors that positively affect the outcome after FHNE (Remedios & Fries 1995, Denny & Butterworth 2000, Schulz & Dejardin 2003).
Aggressive analgesic regimens must be employed in order to alleviate pain as well as ensure the effectiveness of physiotherapy. Therefore, in the immediate postoperative period the use of opioids combined to nonsteroidal anti-inflammatory agents (NSAIDs) is recommended. This treatment may last from a few days to several weeks, depending on its results and afterward only the NSAID is continued until adequate function of the affected limb has been restored (Roush 2012).
In contrast to most orthopaedic procedures, strict confinement of physical activity postoperatively is contraindicated. Instead, controlled physical activity with a gradual increase in duration, is recommended (walks on leash, avoiding running and jumping) as soon as possible after patient recovery (Roush 2012).
Physiotherapy should also begin immediately, and it is recommended to be performed at the time of maximum effect of the analgesic regimen. Daily repeated passive range flexion and extension of the coxofemoral joint is recommended, so that the range of motion can be improved, as well as slow walking, walking at an inclination or on stairs, as well as backward steps with the front limbs of the animal elevated off the ground (Roush 2012). Hydrotherapy, during which the patient moves in water, has a distinct advantage over the exercise on dry land, due to the reduced stress applied on the joints. With hydrotherapy the muscles strengthen and relax, range of motion of the joints is increased, limb function is gradually restored, postoperative oedema is reduced, and local blood perfusion is increased, resulting in faster recovery. The duration of each hydrotherapy session depends on the previous experience of the animal with water, the age, physical condition, body weight and concomitant disorders of other body systems. It is recommended for sessions to occur 2-3 times per week for the first 4-6 weeks (Rivière 2007, Monk 2016) and then 1-2 times per week up to week 12 (Monk 2016), each session lasting for 5-20 min (Rivière 2007). However, there are cases in which hydrotherapy should be avoided. These include infected trauma or surgical sites that have not healed, fever, cardiac, hepatic and renal disorders, hypertension, hypotension, respiratory disorders, infectious diseases (due to transmission), refractory epilepsy and severe generalised muscle weakness (Monk 2016).
Complications
One of the most important complications of FHNE is shortening of the limb (Schulz & Dejardin 2003, Off & Matis 2010), which may be combined with subcutaneous dorsal projection of the greater trochanter. Furthermore, decreased range of motion of the pseudarthrosis may be noted compared to the normal coxofemoral joint, muscle atrophy and reduced limb function (Vasseur 1998). Another complication of FHNE, which is probably due to the change in structure of the coxofemoral joint, is patellar luxation (Berzon et al., 1980, Schulz & Dejardin 2003).
As previously mentioned, extensive damage to the periarticular muscles during the initial injury or surgical manipulations, the erroneous angle followed during ostectomy of the femoral neck and an irregular ostectomy surface can reduce the possibility of satisfactory postoperative results (Berzon et al. 1980).
FHNE was previously considered to be an irreversible surgical procedure. Nowadays it is possible to surgically correct a failed FHNE by total hip replacement arthroplasty, which has been described in both dogs and cats (Liska et al. 2010, Fitzpatrick et al. 2012). Nevertheless, a successful result in this case is particularly difficult to achieve, due to the presence of thick connective tissue between the femoral neck and the acetabulum and periarticular muscle contraction (Young et al. 2015).
Epilogue
FHNE is a simple and fairly inexpensive surgical procedure, with excellent results when the proper surgical technique is employed. There is no doubt that for a lot of patients this is so much more than a “salvage” procedure, considering that it allows them to return to normal life, without pain and with excellent limb function.
Conflict of interests
The authors declare no conflicts of interest.
References
- Ablin LW, Gambardella PC (1991) Orthopaedics of the feline hip. Compend Contin Educ Vet 13, 592–598.
- Berzon JL, Howard PE, Covell E, Trotter J, Dueland R (1980) A retrospective study of the efficacy of femoral head and neck excisions in 94 dogs and cats. Vet Surg 9, 88-92.
- Charnley J (1970) Acrylic Cement in Orthopaedic Surgery. Br J Surg 57, 874.
- Climent S, Latorre R, Kostlin R, Verez-Fraguela J, Sanchez F, Sanchez J, Celdran D (2014) Hip joint. In: 3D Joint Anatomy in Dogs. Servet, Zaragoza, pp. 26-45.
- Coster I, Clarke IE, Moreland J (1981) Surface replacement of the canine hip: An experimental model. J Am Anim Hosp Assoc 17, 181-191.
- DeCamp CE, Johnston SA, Dejardin LM, Schaefer SL (2016) The hip joint. In: Brinker, Piermattei, and Flo’s Handbook of Small Animal Orthopedics and Fracture Repair (5th edn). Elsevier, St Louis, pp. 468–517.
- Denny HR, Butterworth SJ (2000) The hip. In: A Guide to Canine and Feline Orthopedic Surgery (4th edn). Blackwell, Oxford, pp. 455-491.
- Dueland R (1975) Total hip arthroplasty. In: Current Techniques in Small Animal Surgery. Bojrab, MJ. Lea & Febiger, Philadelphia, pp. 448-450.
- Duff R, Campbell JR (1977) Long-term results of excision arthroplasty of the canine hip. Vet Rec 101, 181-184.
- Duff R, Campbell JR (1978) Radiographic appearance and clinical progress after excision arthroplasty of the canine hip. J Small Anim Pract 19, 439-449.
- Fitzpatrick N, Pratola L, Yeadon R, Nikolaou C, Hamilton M, Farelli M (2012) Total hip replacement after failed femoral head and neck excision in two dogs and two cats. Vet Surg 41, 136-142.
- Girdlestone GR (1928) Arthrodesis and other operations for tuberculosis of the hip. In: The Robert Jones Birthday Volume. Milford HW. Oxford University Press, London, pp. 347–374.
- Girdlestone GR (1943) Acute pyogenic arthritis of the hip: an operation giving free access and effective drainage. Lancet 241, 419- 421.
- Harasen G (2004) The femoral head and neck ostectomy. Can Vet J 45, 163-164.
- Harper TAM (2017) Femoral head and neck excision. Vet Clin Small Anim 47, 885-897.
- Hofmeyr CFB (1966) Excision arthroplasty for canine hip lesions. Mod Vet Pract 47, 56-58.
- Johnson AL, Hulse DA (2001) Diseases of the joints. In: Small Animal Surgery. Fossum TW (2nd edn). Mosby, St. Louis, pp. 1093- 1109.
- Johnson KA (2014a) The hindlimb. Approach to the craniodorsal aspect of the hip joint through a craniodorsal incision in the dog. In: Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat (5th edn). Elsevier, St Louis, pp 322-327.
- Johnson KA (2014b) The hindlimb. Approach to the craniodorsal aspect of the hip joint through a craniodorsal incision in the cat. In: Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat (5th edn). Elsevier, St Louis, pp. 328-335.
- Lee R, Fry PD (1969) Some observations on the occurance of Legg- Calvé-Perthes’ disease (Coxaplana) in the dog, and an evaluation of excision arthroplasty as a method of treatment. J Small Anim Pract 10, 309-317.
- Lewis DD, Bellah JR, McGavin MD, Gaskin JM (1988) Postoperative examination of the biceps femoris muscle sling used in excision of the femoral head and neck in dogs. Vet Surg 17, 269-277.
- Liska WD, Doyle ND, Schwartz Z (2010) Successful revision of a femoral head ostectomy (complicated by postoperative sciatic neurapraxia) to a total hip replacement in a cat. Vet Comp Orthop Traumatol 23, 119-123.
- Ljunggren G (1967) Legg-Perthes disease in the dog. Acta Orthop Scand 95, 1-79.
- Manley PA (1993) The hip joint. In: Textbook of Small Animal Surgery. Slatter D (2nd edn). WB Saunders, Philadelphia, pp. 1798–1799.
- Mann FA, Tangner CH, Wagner-Mann C, Read WK, Hulse DA, Puglisi TA, Hobson HP (1987) A comparison of standard femoral head and neck excision and femoral head and neck excision using a biceps femoris muscle flap in the dog. Vet Surg 16, 223-230.
- Mann FA, Hathcock JT and Wagner-Mann C (1993) Estimation of soft tissue interposition after femoral head and neck excision in dogs using ventrodorsal pelvic radiography. Vet Radiol Ultrasound 34, 230-234.
- Monk M (2016) Aquatic therapy. In: Animal Physiotherapy Assessment, Treatment and Rehabilitation of Animals. McGowan CM, Goff L (2nd edn). Wiley Blackwell, West Sussex, pp. 225-237.
- Montgomery RD, Milton JL, Horne RD, Coble RH, Williams JC (1987) A retrospective comparison of three techniques for femoral head and neck excision in dogs. Vet Surg 16, 423-426.
- Off W, Matis U (2010) Excision arthroplasty of the hip joint in dogs and cats: Clinical, radiographic, and gait analysis findings from the Department of Surgery, Veterinary Faculty of the Ludwig- Maximilians-University of Munich, Germany. Vet Comp Orthop Traumatol 23, 297-305.
- Olmstead ML, Hohm RB, Turner TM (1983) A five-year study of 221 total hip replacements in the dog. J Am Vet Med Assoc 183, 191-194.
- Ormrod AN (1961) Treatment of hip lameness in the dog by excision of the femoral head. Vet Rec 73, 576-577.
- Piek CJ, Hazewinkel HAW, Wolvekamp WTC, Nap RC, Mey BP (1996) Long term follow-up of avascular necrosis of the femoral head in the dog. J Small Anim Pract 37, 12-18.
- Plante J, Dupuis J, Beauregard G, Bonneau NH, Breton L (1997) Long term results of conservative treatment, excision arthroplasty and triple pelvic osteotomy for the treatment of hip dysplasia in the immature dog, part 2: analysis of the ground reaction forces. Vet Comp Orthop Traumatol 10, 130–135.
- Prostredny JM (2014) Excision arthroplasty of the femoral head and neck. In: Current techniques in small animal surgery. Bojrab MJ (5th edn). Teton New Media, Jackson, pp. 1048-1052.
- Prostredny JM, Toombs JP, VanSickle DC (1991) Effect of two muscle sling techniques on early morbidity after femoral head and neck excision in dogs. Vet Surg 20, 298-305.
- Rawson EA, Aronsohn MG, Burk RL (2005) Simultaneous bilateral femoral head and neck ostectomy for the treatment of canine hip dysplasia. J Am Anim Hosp Assoc 41, 166-170.
- Remedios AM, Fries CL (1995) Treatment of canine hip dysplasia: a review. Can Vet J 36, 503-509.
- Rex MAE (1963) Spreull’s excision arhtroplasty of the hip joint in the dog and cat. Austr Vet J 39, 275-278.
- Rivière S (2007) Physiotherapy for cats and dogs applied to locomotor disorders of arthritic origin. Veterinary Focus 17, 32-36.
- Roush JK (2012) Surgical Therapy of Canine Hip Dysplasia In: Veterinary Surgery Small Animal. Tobias KM, Johnston SA. (2nd edn.). Saunders, St. Louis, pp. 849-864.
- Schulz KS and Dejardin LM (2003) Surgical treatment of canine hip dysplasia. In: Textbook of Small Animal Surgery. Slatter D (3rd edn). Elsevier, Philadelphia, pp. 2029-2059.
- Schulz KS (2012) Diseases of the joints In: Small Animal Surgery. Fossum TW (4th edn). Elsevier Mosby, St Louis, pp.1305-1316.
- Seer G, Hurov R (1968) Simultaneous bilateral coxofemoral excision arhtroplasty in the dog. Can Vet J 9, 70-73.
- Spruell JSA (1961) Excision arthroplasty as a method of treatment of hip joint disease in the dog Vet Rec 73, 573-576.
- Vasseur PB (1998) Femoral head and neck ostectomy. In: Current Techniques in Small Animal Surgery. Bojrab MJ (4th edn). Lea & Febiger, Philadelphia, pp. 1170-1173.
- Wallace LJ, Olmstead ML (1995) Disabling conditions of the canine coxofemoral joint. In: Small Animal Orthopedics. Olmstead ML. Mosby-Year Book, St. Louis, pp. 361-393.
- Young Heo S, Won Seol J, Beom Lee H (2015) Total hip replacement in two dogs with unsuccessful femoral head ostectomy. J Vet Sci 16, 131-134.
Corresponding author:
Androniki Krystalli
e-mail: This email address is being protected from spambots. You need JavaScript enabled to view it.
