

> Abstract
Elbow hygroma is a serous fluid accumulation over the olecranon caused by repetitive trauma in dogs lying on hard surfaces during housing. Diagnosis is made by physical examination and fi ne needle aspiration of the hygroma cavity. Treatment may be conservative or surgical. Padded bandages and soft bedding are provided for small hygromas until the formation of a callus. Surgical intervention in reserved for recurrent, large or complicated hygromas and includes drainage or surgical excision.
> Definition and clinical signs
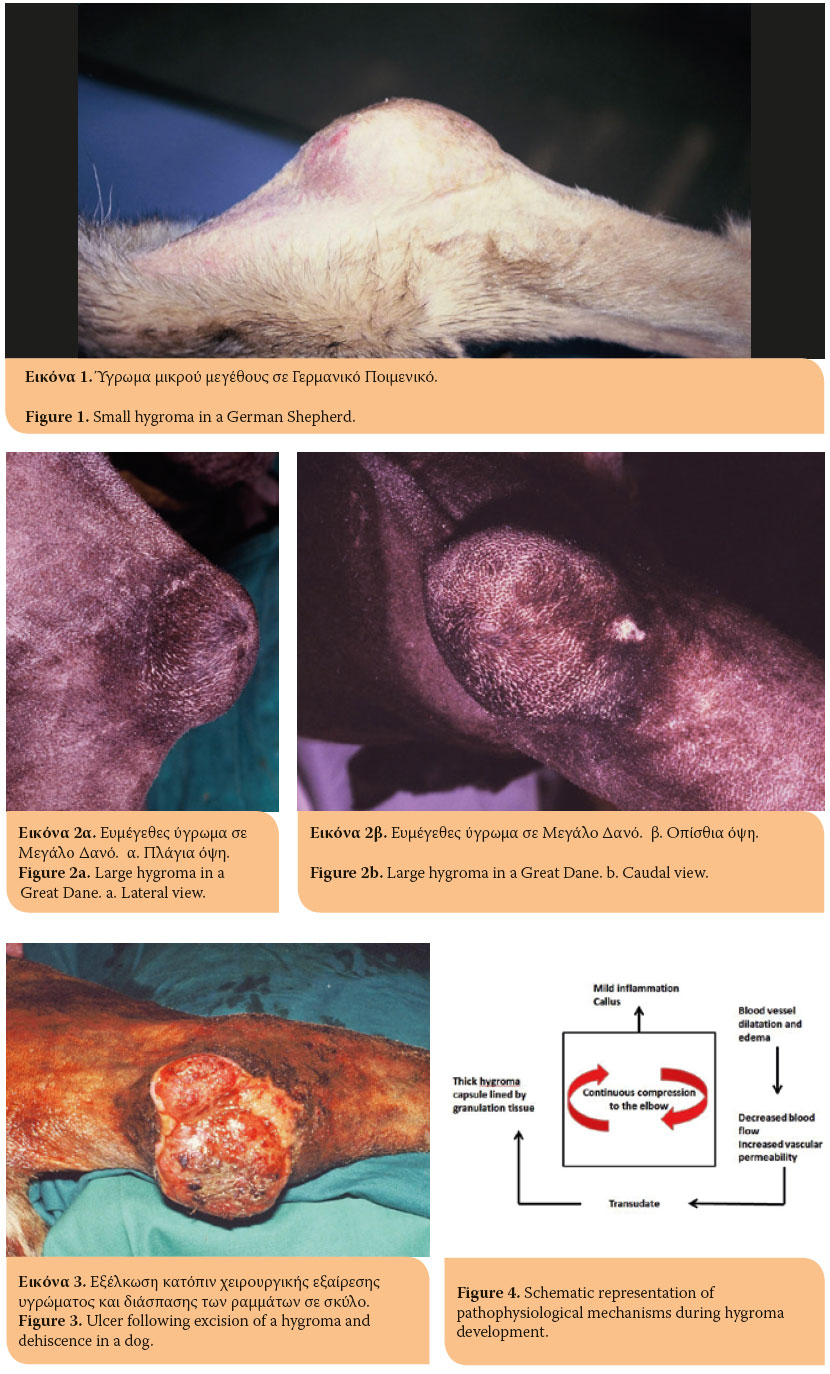
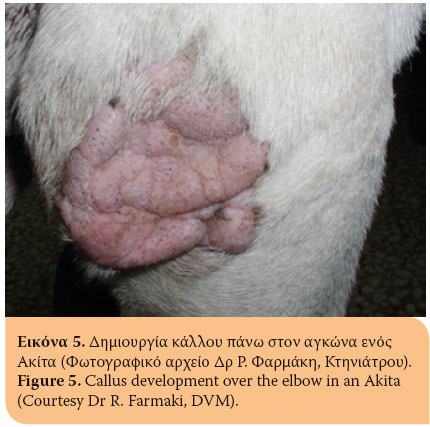
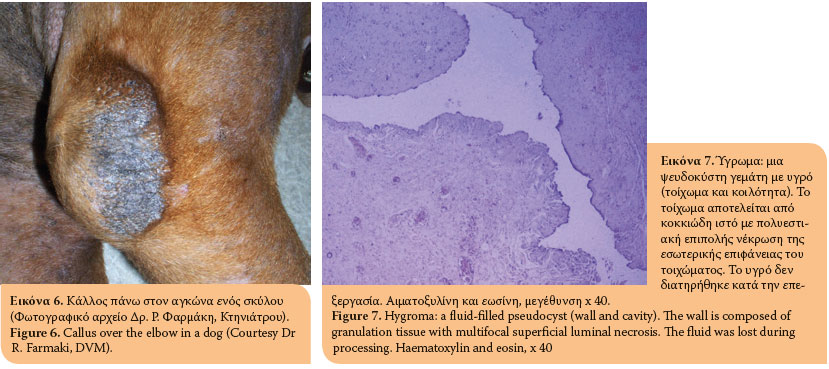
Elbow hygroma is a chronic subcutaneous serous fl uid collection resulting from continuous trauma to soft tissues over the olecranon in dogs lying on hard surfaces during housing (Figure 1).1-6 It commonly occurs in large or giant breeds of dogs (Great Danes, St Bernards, Mastiffs, Weimeraners, German shepherds, Irish Wolfhounds and Newfounlands), aged between 6 and 18 months (Figure 2).4,5 Most hygromas are small and painless. They do not generally involve the elbow joint and can be unilateral or bilateral. Repeated trauma causes enlargement of the hygroma and thickening of its capsule. The skin may become ulcerated over the hygroma (Figure 3).6
> Pathophysiology
The olecranon is a bony prominence covered by multiple layers of soft tissue including the periosteum, deep fascia, fat, loose connective tissue and skin. The application of pressure over the olecranon is transmitted from the skin to the underlying bone leading to variable compression of soft tissues.7 Measurements of sitting pressure on the skin covering the ischial tuberosity in humans has been found to exceed 300 mm Hg. This pressure exceeds the normal range of 12 –70 mm Hg in skin capillaries. Repeated pressure of soft tissues surrounding the olecranon can occlude blood supply and result in ischaemic necrosis.8
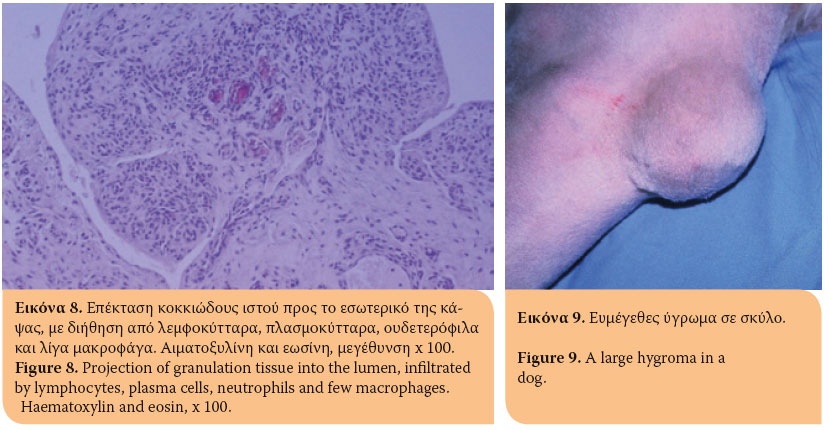
 The mechanism of hygroma development can be divided into five stages (Figure 4).2,5,7,8 In most dogs, repeated trauma over the olecranon leads to protective callus formation (Figures 5, 6). This process is characterized by mild inflammation with minimal tissue destruction.
The mechanism of hygroma development can be divided into five stages (Figure 4).2,5,7,8 In most dogs, repeated trauma over the olecranon leads to protective callus formation (Figures 5, 6). This process is characterized by mild inflammation with minimal tissue destruction.
Stage 1
In cases where a callus is not formed, a grade I pressure sore develops that is characterized by erythema as a result of blood vessel dilatation and oedema.
Stage 2
If compression continues, local ischaemia develops due to impairment of vascular flow. This causes oedema and transudate formation.
Stage 3
When trauma persists, the inflammatory response is marked; the tissues surrounding the transudate become ischaemic and the transudate is not absorbed but is enclosed in a thick capsule lined by granulation tissue.
Stage 4
The inflammatory response worsens, and fluid accumulation becomes more intense and is associated with chronic infl ammatory tissue. Repetitive episodes of trauma lead to a vicious cycle perpetuating the chronic inflammatory response.
Stage 5
Stretching of the skin overlying the hygroma may lead to ulceration and infection.
Macroscopically, loose connective tissue is formed between the overlying skin and the hygroma. The hygroma cavity is enclosed by a dense connective capsule that contains yellow to red mucinous fl uid compatible with transudate. The lining of the capsule is pale and smooth or rough, with villus-like tissue projections into the lumen.1,2
> Histopathology
The wall of the capsule is lined by granulation tissue with high collagen content. Granulation tissue lining is irregular due to the villus-like projections (Figures 7, 8). The hygroma capsule lining is not secretory; hence, it is not considered a true cyst.1
> Diagnosis
Diagnosis of hygroma is based on the history and physical examination fi ndings. Diff erential diagnosis includes abscesses and neoplasms. Fine needle aspiration and cytology helps in differentiation. An orthopaedic consultation for further investigation and management of possible hip pathology that may result in excessive weight-bearing on the elbows during sternal recumbency should also be sought.5,9
> Treatment
Identifi cation and removal of the underlying cause is the gold standard for hygroma management. There is a paucity of information in the veterinary literature concerning treatment of hygromas. The number of cases reported over the years is relatively low.1,2 This could be ascribed to the fact that most owners pursue a conservative approach early in the disease process with favourable results, and only a few cases undergo surgical treatment. In consequence, no studies have been undertaken to compare the existing surgical techniques.
> Conservative treatment
The goal of treatment is to reduce repetitive trauma and provide protection to the elbow to allow healing of the granulation tissue.9 Initially, conservative treatment should be undertaken for all small hygromas.4,5,6 Padded bandages and soft bedding are eff ective in most dogs with small hygromas if encountered early in the course of the disease.5,6 Adjustable neoprene sleeves provide long-term protection of the elbows; they are easy to use and are well tolerated by most dogs.6 Following conservative management, most hygromas resolve as infl ammatory reaction decreases and granulation tissue becomes fi brotic.5 Finally, a callus develops over the olecranon providing lifelong protection for the elbow.4 Repeated aspiration or infusion of corticosteroids in the hygroma cavity should be discouraged since a risk of recurrence or bacterial contamination could be incurred, resulting in infection and abscess formation within the cavity.5,10
> Surgical treatment
Indications
The indications for surgical management of hygromas include hygromas that do not respond to conservative treatment, chronic or large hygromas with a thick capsule (Fig 9), infected or ulcerated hygromas, and cases of recurrence.4,5
Surgical treatment includes drainage and complete surgical excision. Drainage with passive or closed suction systems gradually obliterates the hygroma cavity by granulation tissue formation and subsequent fi brosis. However, the remaining granulation tissue may lead to recurrence. Partial debridement of granulation tissue followed by apposition of the hygroma capsule edges with sutures seems not to provide a rational approach to hygroma management.1,5 In contrast, complete surgical excision addresses all problematic granulation tissue that is responsible for transudate formation in the hygroma cavity.5 Surgical excision and first intention healing entails removal of all granulation tissue, thus reducing the possibility of recurrence associated with further trauma. Infected or ulcerated hygromas usually require some form of reconstructive surgery. Many authors are against surgical excision of hygromas as they believe that it could lead to serious complications including dehiscence and ulceration2,4-6,9,11,12
> Penrose drains or closed suction drainage
Following surgical preparation of the elbow area, stab incisions are made at the proximal and distal borders of the hygroma. The fluid is drained and all fi brin debris is removed. One or two ¼ inch Penrose drains are inserted through the incisions and secured in place with sutures (Figure 10). A non-adherent dressing is applied to the wound, and the limb is supported with a Robert Jones bandage to be changed every five days (Figure 11). Penrose drains are removed after 3-4 weeks at the time of the last bandage change. Latex Penrose drains cause a mild infl ammatory reaction that converts the chronic infl ammatory process to acute, thus giving rise to fi brosis. At the same time, the Robert Jones bandage keeps the walls of the cavity in apposition.2,4,11 A closed suction drain can also be placed through one or two incisions at the distal and proximal borders of the hygroma in such a fashion as to accommodate the whole fenestrated drain following a subcutaneous course at the skin distal to the hygroma (Figure 12). Duration of drainage is 3 - 4 weeks. The major advantage of closed suction drainage is that bandaging is not required.4,13 In one study, Penrose drainage was used in 18 hygromas of 12 dogs; no postoperative complications were reported after two years of follow-up.2 Redundant skin over the olecranon of large hygromas diminishes over time.


> Surgical excision
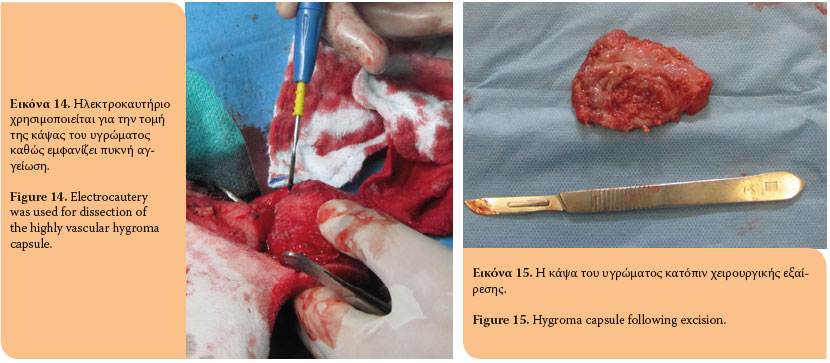
A skin incision is made medial or lateral to the elbow in order to avoid the bony prominence, thus preventing wound tension and dehiscence (Figure 13).5 The highly vascular capsule is separated from the soft tissues and underlying bone using electrocautery or blunt dissection (Figures 14, 15). Perforation of the hygroma cavity and spillage of the transudate may be encountered during dissection, but it is of minor clinical signifi cance. Following hygroma removal, dead space obliteration is achieved with multiple layers of synthetic absorbable monofi lament 3/0 suture material and the skin is closed with 3/0 nylon (Figures 16, 17). A Robert Jones bandage is placed to support the limb, and bandage changes are regularly performed until suture removal.5 No attempt is made to remove loose skin over the elbow (Figures 18, 19). Wound dehiscence and ulceration are potential complications.2
> Management of complicated hygromas
In the event of infected but not ulcerated hygromas, culture and sensitivity test of the aspirated fluid should be performed and the appropriate antimicrobial treatment instituted before surgical excision is attempted.5
Failure of conservative management or infection and dehiscence following excision of the hygroma may lead to ulcer development over the olecranon.6 These ulcers are difficult to manage because of the insufficient skin available for coverage and increased tension during flexion of the elbow.2 Second intention healing is not an option since it will never result in complete healing. Small ulcerated hygromas can be managed by surgical excision and reconstruction with an advancement flap.2,3,4 Larger ulcers may be reconstructed with a transposition or thoracodorsal axial pattern flap (Figures 20, 21).4,11,12

> Βιβλιογραφία
1. Newton CD, Wilson GP, Allen HL, Swenberg JA. Surgical closure of elbow hygroma in the dog. J Am Vet Med Assoc 1974, 164: 147-149.
2. Johnston DE. Hygroma of the elbow in dogs. J Am Vet Med Assoc 1975, 167: 213-219.
3. Johnston DE. Hygroma of the elbow in dogs. Comp Contin Educ Pract Vet 1979, 1: 157-162.
4. Pope ER. Surgical treatment of hygroma of the elbow. In: Current Techniques in Small Animal Surgery. Bojrab MJ (ed). 4th edn. Williams and Wilkins: Baltimore, 1998, pp. 622-625.
5. White RAS. Surgical treatment of specifi c skin disorders. In: Textbook of Small Animal Surgery. Slatter D (ed). 3rd edn. Saunders: Philadelphia, 2003, pp. 339-355.
6. Pavletic MM. Management of specifi c wounds. In: Atlas of Small Animal Wound Management and Reconstructive Surgery. Pavletic MM (ed). 3rd edn. Wiley-Blackwell: Ames, 2010, pp. 159- 229.
7. Toomey AA, Bojrab MJ. Hygroma of the elbow. In: Current Techniques in Small Animal Surgery. Bojrab MJ (ed). 2nd edn. Lea and Febiger: Philadelphia, 1983, pp. 443-446.
8. Johnston DE. Bursitis and Tendinitis. In: Disease Mechanisms in Small Animal Surgery. Bojrab MJ (ed). 2nd edn. Lea and Febiger: Philadelphia, 1993, pp. 1089-1093.
9. Lanz OI, Waldron DR. Elbow Hygroma. In: Clinical Veterinary Advisor. Cote E (ed). 3rd edn. Elsevier: St Louis, 2015, pp. 310-311.
10. Canapp SO, Campana DM, Fair LM. Orhopedic coaptation devices and small- animal prosthetics. In: Veterinary Surgery Small Animal. Tobias km, Johnston SA (eds). Elsevier: St Louis, 2012, pp. 628-646.
11. Swaim SF, Henderson RA. Wounds on limbs. In: Small Animal Wound Management. Swaim SF, Henderson RA (eds). 2nd edn. Williams and Wilkins: Baltimore, 1997, pp. 295-304.
12. Pope ER, Swaim SF. Chronic elbow ulceration repair utilizing an axial pattern fl ap based on the thoracodorsal artery J Am Anim Hosp Assoc 1986, 22: 89-93.
13. Pavletic MM, Brum DE. Succesful closed suction drain management of a canine elbow hygroma. J Small Anim Pract 2015, 56: 476-479.
