

> Abstract
Τhe cause and pathophysiology of hiatal hernia are not yet fully understood, but hiatal hernia seldom appears in dogs and is rarer in cats. Sliding hiatal hernia is the most common type to present in clinical practice. Chinese Shar-Pei dogs are predisposed to the development of this type of hernia. The majority of clinical signs are due to gastroesophageal reflux. Diagnosis is based on diagnostic imaging, and esophagoscopy may provide useful information. It can be managed medically and surgically. The aim of surgical treatment is the anatomical repair and stabilization of the hernia. Prognosis for patients with hiatal hernia is usually favorable.
The aim of this review is to describe the etiology, pathophysiology and treatment of hiatal hernia in companion animals.
> CLASSIFICATION
Hernia of the esophageal hiatus or hiatal hernia (HH) is the condition in which organs of the abdominal cavity herniate through the esophageal hiatus into the thoracic cavity. Hiatal hernia seldom appears in dogs and is rarer in cats. 1,2 Four types of HH have been described. Classification of HH in animals is characterized by ambiguity but follows the classification that is used for humans.1-5
Type I
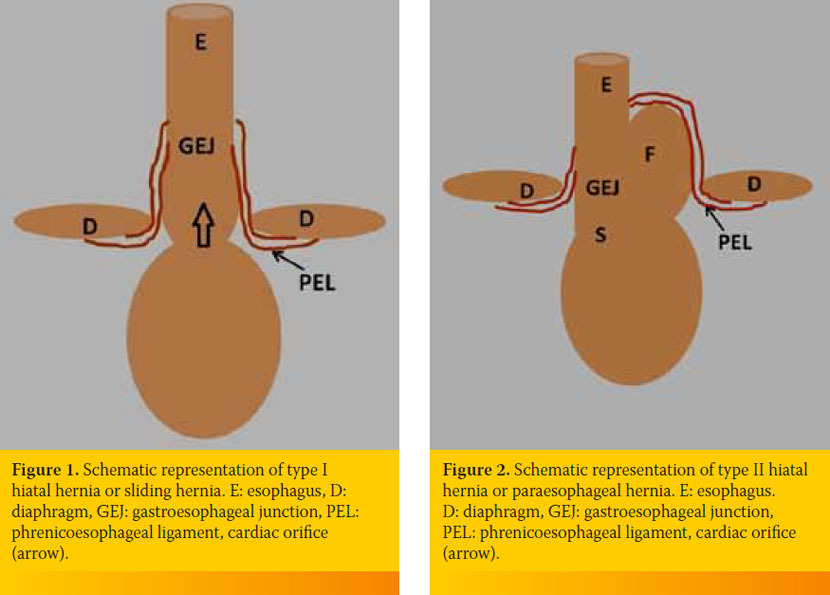
Type I or sliding HH is characterized by the dynamic and intermittent prolapse of the distal part of the esophagus, the gastroesophageal junction and part of the stomach through the esophageal hiatus into the thoracic cavity (Figure 1). Sliding HH occurs more frequently in companion animals than other types of HH and is the most common type of HH to be described in cats.6-24
Type II
Type II or paraesophageal HH is defined by the prolapse of the fundic region of the stomach into the thoracic cavity alongside the thoracic esophagus, while the gastroesophageal junction remains in its normal position (Figure 2). Paraesophageal hernia has been reported in three dogs,25-27 and paraesophageal hernia with prolapse only of the omentum in the thoracic cavity has been described in one cat.28
Type III
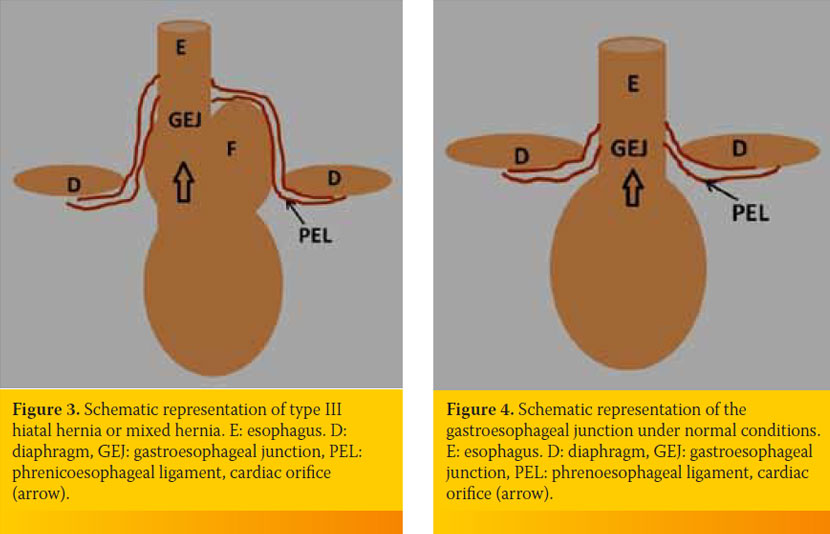
Type III or mixed HH is a combination of types I and II and has been reported in two dogs (Figure 3).4,29
Type IV
Type IV represents a type III HH, accompanied by prolapse of the stomach, liver and other abdominal organs into the thoracic cavity, and has been described in three dogs.30-32 Generally, HH may be of a permanent or dynamic nature, depending on changes in the position of the animal and of the intrathoracic pressure.1 Knowledge of the various types of HH is necessary since each type is accompanied by a different pathophysiology and symptomatology and requires different treatment.3,4,25
> SURGICAL ANATOMY AND FUNCTIONAL REMINDER OF GASTROESOPHAGEAL JUNCTION
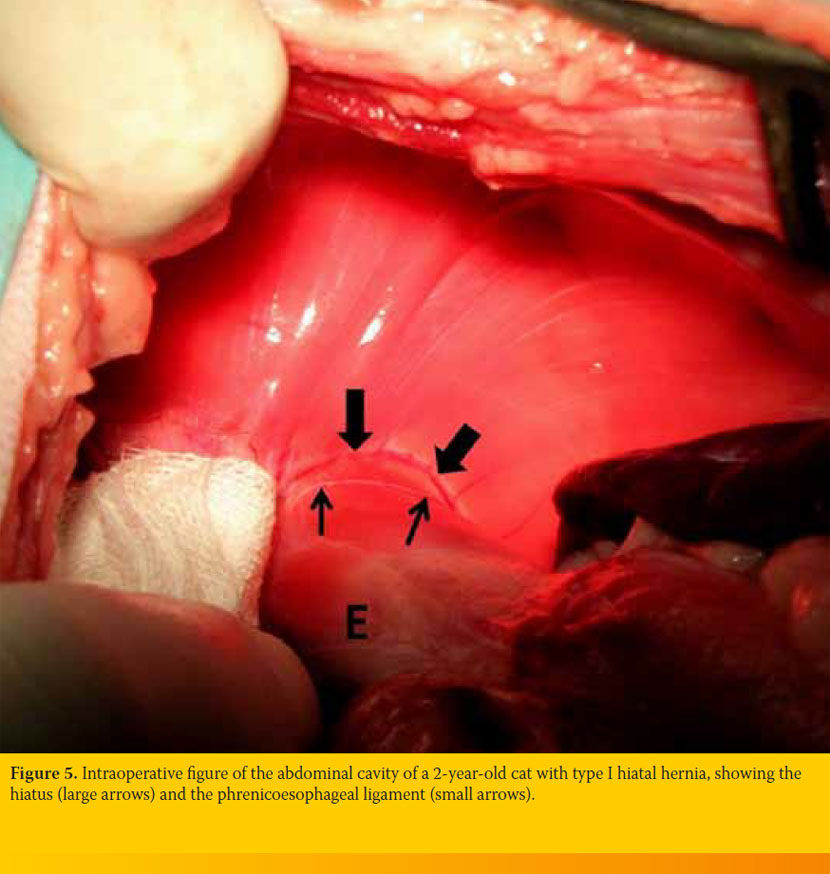
The esophageal hiatus is an opening of the diaphragm which is located ventral to the aortic foramen and on the right of the midline, through which the esophagus passes in order to enter the abdominal cavity. The gastroesophageal junction constitutes the anatomical region where the esophagus transits to the stomach. Normally it is located at the intra-abdominal portion of the esophagus. The esophagus is connected to the esophageal hiatus through the phrenicoesophageal ligament, which impedes movement of the abdominal part of the esophagus to the thoracic cavity (Figure 4). The phrenicoesophageal ligament of the cat differs from that of the dog in that its descending limb is attached to the esophagus below the esophagogastric angle and its esophageal
attachments are more superficial (Figure 5).33 The caudal esophageal sphincter constitutes a high-pressure zone and indistinct anatomical region, extending from the hiatus to the gastric cardia in both dogs and cats.34-35 Histologically, the caudal esophageal sphincter of the dog consists of striated muscle fibers, as opposed to the smooth muscle fibers in the cat.33
It is argued that the intra-abdominal esophagus receives greater extrinsic pressure, resulting in prevention of gastroesophageal reflux (GER). This view is disputed in dogs since it has been shown that the intra-abdominal portion of the esophagus is absent in a few breeds.36,37 It is as yet unknown whether the intra-abdominal portion of the esophagus exists in cats. Maintenance of high pressure and prevention of GER are considered to be controlled by exogenous factors such as the small length of the intra-abdominal portion of the esophagus, the right side of the diaphragm which surrounds the intra-abdominal portion of the diaphragm as a lasso, the phrenicoesophageal ligament, the cardiac orifice of the stomach, the maintenance of the acute esophagogastric angle, and the site of recumbency of the dog.3,36,38
> ETIOLOGY, PATHOPHYSIOLOGY AND PREDISPOSING FACTORS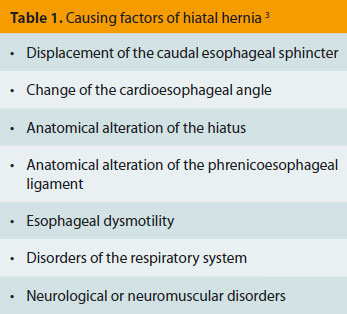 Hiatal hernia is a disease with uncertain etiology and pathophysiology, which is characterized by the interaction of many factors (Table 1).3 Most of the information available on the pathophysiology of HH in companion animals is derived from studies in humans; it is suggested that the pathophysiology of the dog and human are similar.3
Hiatal hernia is a disease with uncertain etiology and pathophysiology, which is characterized by the interaction of many factors (Table 1).3 Most of the information available on the pathophysiology of HH in companion animals is derived from studies in humans; it is suggested that the pathophysiology of the dog and human are similar.3
In dogs with HH, the gastroesophageal junction is displaced cranially, resulting in disruption of exogenous factors, which control the pressure of the caudal esophageal sphincter and the development of esophagitis due to GER, which also causes the symptomatology of HH. However, the reason why many animals with HH remain asymptomatic remains unknown.12,16 It can possibly be ascribed to the presence of protective mechanisms that prevent esophagitis, such as the small exposure time of the esophageal lumen to the reflux content, the neutralization of the content of saliva bicarbonates and the histological structure of the esophageal mucosa, which appears to be stronger in these animals.39 Moreover, contrary to previous beliefs, there is no primary inadequacy (achalasia) of the caudal esophageal sphincter in the dog.3 Congenital HH, and more specifically Type I, is the most frequent form. Observed in brachycephalic breeds, and especially in English Bulldogs and Shar-Peis, it is probably due to abnormal closure of the diaphragm during fetal life. 15,16,18,22,40-42 A strong association between obstruction of the upper respiratory system and esophagitis due to GER has been reported in brachycephalic breeds.41,42 Inspiratory dyspnea caused by obstruction of the upper respiratory system, which is observed in brachycephalic breeds, mainly in English bulldogs but also in other breeds of dogs and cats, could lead to an increase in negative intraesophageal and intrapleural pressure, resulting in the development of HH and the movement of the gastroesophageal junction and stomach into the thoracic cavity, and the development of relevant symptomatology.10,18,24,41-44 Hiatal hernia can also occur as a complication of corrective surgery of the diaphragmatic hernia because of injury or increased pressure at the site of the hiatus and in changes in the activity of the vagus nerve due to surgical injury.10,12,13,17 Tetanus in dogs was related to the presence of HH due to neuromuscular dysfunction of the diaphragm, the gastroesophageal junction and the abdominal wall, resulting in convulsion of the diaphragm, esophageal dysmotility and the development of HH.45,46 Hiatal hernia may also be related to the presence of dysmotility of the esophagus, megaesophagus and even esophageal lumen stenosis, because of esophagitis caused by GER in both dogs and cats.12,13,15,16,18,19 As concerns Type II or paraesophageal hernia, it is rarely accompanied by esophagitis due to GER, unless it coexists with sliding hernia or megaesophagus (Types III and IV).4,26,27,32
> CLINICAL FINDINGS
before the age of 12 months, while in cats the diagnosis is made more frequently in animals older than 12 months.10,12,15,22 In some animals, HH does not present any clinical symptomatology.12,16 In Type I HH, the clinical findings are more often associated with GER and include regurgitation, vomiting, hypersalivation, hematemesis, weight loss and respiratory distress. 10,12,15,22 In Types IIIV HH, clinical findings more frequently involve respiratory distress, depression or collapse. 25-27,30,32 The Budd-Chiari syndrome was observed in a Shar-Pei dog with Type IV HH, due to compression of the caudal vena cava from the transposed left liver lobe.31
> DIAGNOSIS
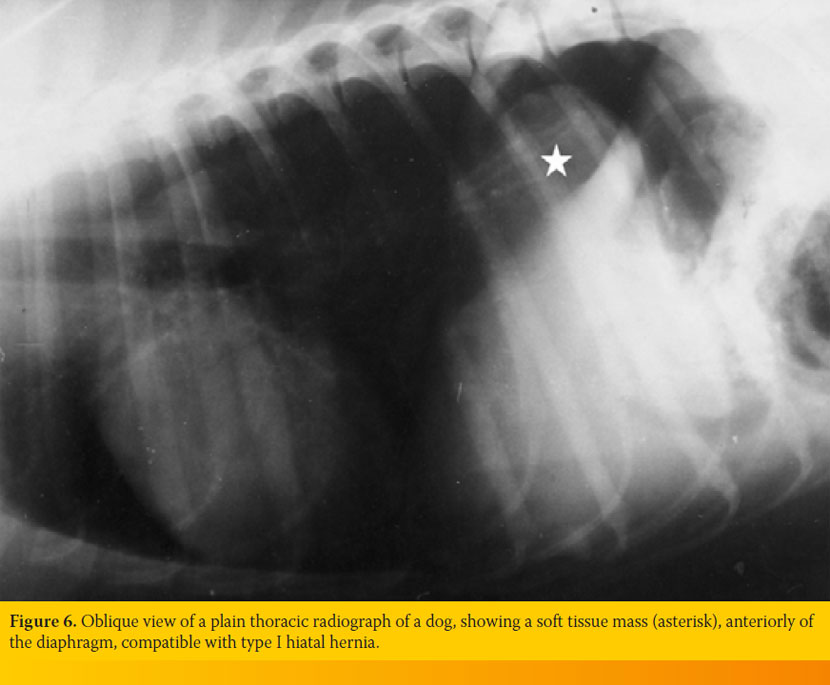
Confirmation of diagnosis is made with radiographic imaging of the thorax and esophagography, with or without fluoroscopy, after consumption of a barium meal. 2,10,12,15,16 A soft tissue mass or gas-filled mass in the caudal portion of the thoracic region of the esophagus (epiphrenic mass), megaesophagus and aspiration pneumonia are observed in plain thoracic radiographs (Figure 6). 10,12,15,16
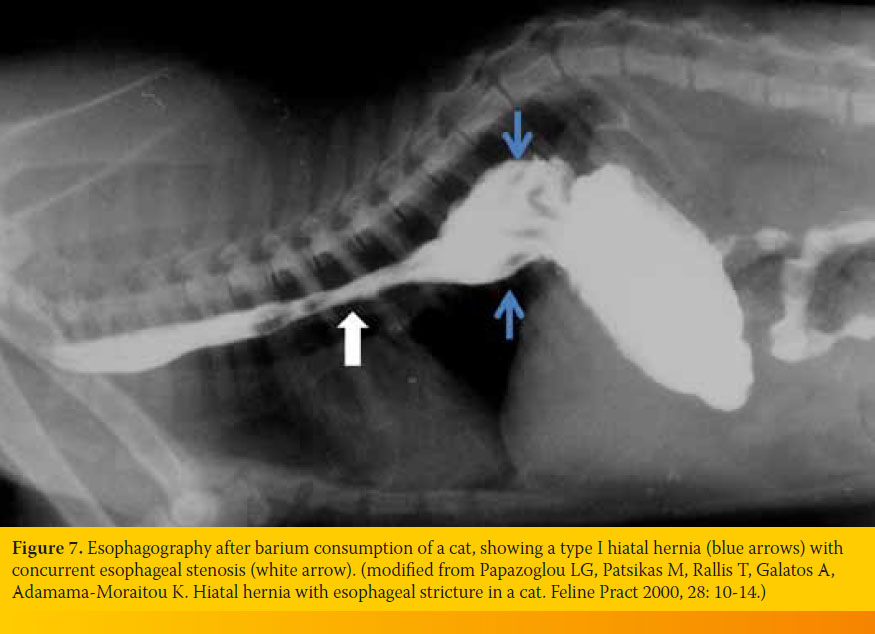
Differential diagnosis must include esophageal diverticulum, gastroesophageal intussusception, tumors and foreign bodies.2 Esophagography following consumption of a barium meal may facilitate the differential diagnosis of Type I HH from Type II, and will show cranial displacement of gastroesophageal junction, retention of barium in the dilated caudal region of the esophagus and imaging of aspects of the stomach (Figure7). 10,12,15,16 Esophagography will reveal GER, displacement of the gastroesophageal junction and esophageal dysmotility. 12,15,16 Esophagoscopy performed with a flexible endoscope will help us see the distension of the hiatus, esophagitis and GER.2
> TREATMENT
Medical management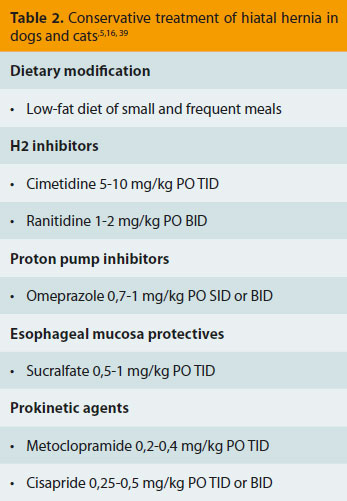 Congenital Type I HH can be treated both medically and surgically with very good results. 11,12,14-16,22 However, there is disagreement among the surgeons concerning the decision for surgical or conservative treatment. Some surgeons recommend immediate surgical treatment for Shar-Pei dogs since most animals of this breed do not seem to respond to medical treatment. 15,22,47 Whatever the case, the treatment of the primary cause contributes to the resolution of symptoms. 2,41,42 Conservative treatment generally aims to treat the symptoms of esophagitis and GER. More specifically, the intention of medical treatment is the reduction of the volume of refluxate secretion and elevation of the pH of the gastric fluid, protection of the esophageal mucosa from inflammation and ulcers and acceleration of gastric evacuation with the concurrent increase in tone of the caudal esophageal sphincter. 2,12,16 This is accomplished by administering a low-fat diet of frequent meals, H2 inhibitors or inhibitors of the proton pump, gastroprotective and prokinetic agents. In the case of megaesophagus, the animal should be fed from a height. According to one study, 8 out of 15 dogs and cats with congenital Type I HH will resolve following conservative treatment.16 No treatment is needed for animals that do not show any clinical symptomatology.12 No GER is observed in Type II HH because the caudal esophageal sphincter remains in place. In this type of hernia, the symptomatology is due to prolapse of the stomach or other organs into the thoracic cavity; hence, surgical treatment is always required. 25,26,28 However, the presence of megaesophagus and secondary GER is an exception and requires a combination of medical and surgical treatment.27
Congenital Type I HH can be treated both medically and surgically with very good results. 11,12,14-16,22 However, there is disagreement among the surgeons concerning the decision for surgical or conservative treatment. Some surgeons recommend immediate surgical treatment for Shar-Pei dogs since most animals of this breed do not seem to respond to medical treatment. 15,22,47 Whatever the case, the treatment of the primary cause contributes to the resolution of symptoms. 2,41,42 Conservative treatment generally aims to treat the symptoms of esophagitis and GER. More specifically, the intention of medical treatment is the reduction of the volume of refluxate secretion and elevation of the pH of the gastric fluid, protection of the esophageal mucosa from inflammation and ulcers and acceleration of gastric evacuation with the concurrent increase in tone of the caudal esophageal sphincter. 2,12,16 This is accomplished by administering a low-fat diet of frequent meals, H2 inhibitors or inhibitors of the proton pump, gastroprotective and prokinetic agents. In the case of megaesophagus, the animal should be fed from a height. According to one study, 8 out of 15 dogs and cats with congenital Type I HH will resolve following conservative treatment.16 No treatment is needed for animals that do not show any clinical symptomatology.12 No GER is observed in Type II HH because the caudal esophageal sphincter remains in place. In this type of hernia, the symptomatology is due to prolapse of the stomach or other organs into the thoracic cavity; hence, surgical treatment is always required. 25,26,28 However, the presence of megaesophagus and secondary GER is an exception and requires a combination of medical and surgical treatment.27
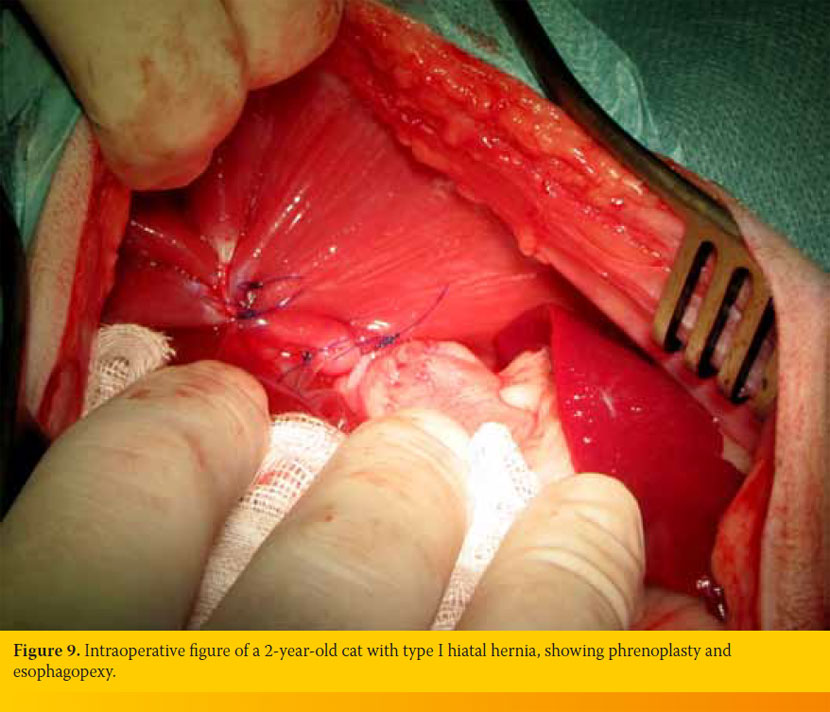
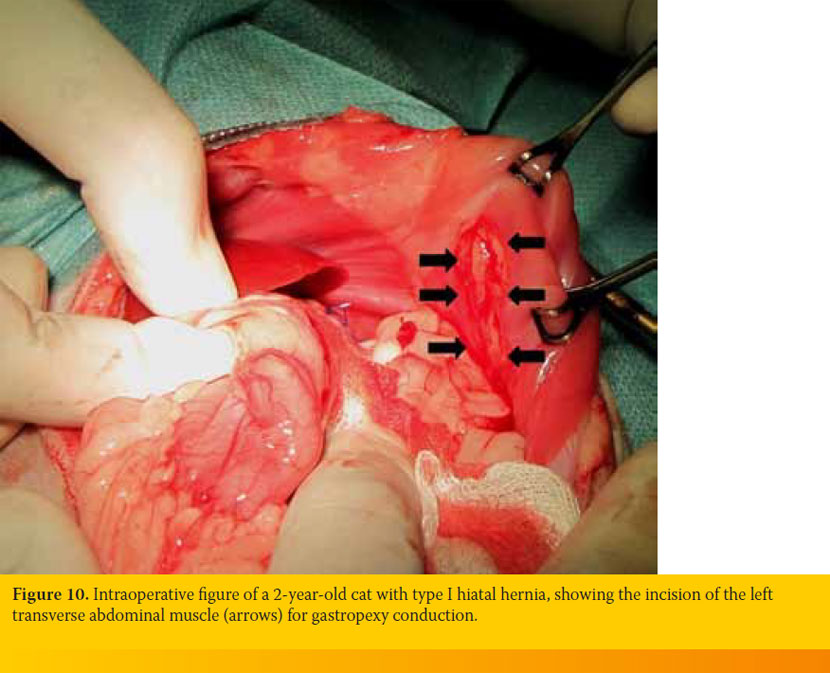
Surgical treatment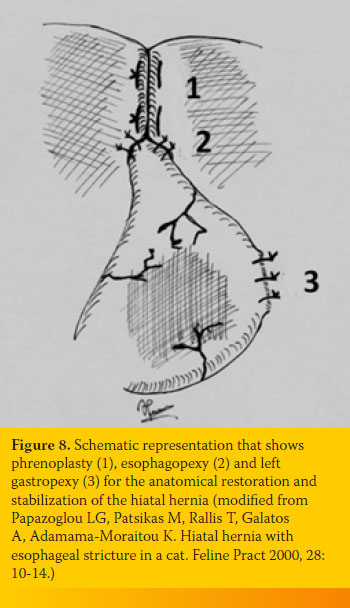 Surgical treatment of HH is indicated if conservative treatment, which lasts 30 days, fails in type II-IV hernias and in Shar-Pei dogs. 12,15,16,22,47 Previously, surgical treatment of HH aimed to strengthen the caudal esophageal sphincter, which was considered to have failure or achalasia, with the use of various fundoplication techniques. These techniques were characterized by a high complication rate, and were abandoned because the theory of achalasia was eliminated.6,10-12,16 Nowadays, the surgical treatment of choice is the anatomical restoration and stabilization of HH.11 This surgery guarantees the best results with the use of the simplest surgical techniques. The surgery aims at the reduction in the hiatus diameter (phrenoplasty), fixation of the esophagus to the diaphragmatic crus with esophagopexy, and fixation of the stomach to the left abdominal wall with gastropexy (Figure 8).11 In the case of aspiration pneumonia, appropriate antibiotherapy should be administered preoperatively. The hiatus is approached through a median laparotomy after the passage of an orogastric tube through the esophagus to allow easier identification of the esophagus and hiatus: the hepatic ligament is transected, the left liver lobes are retracted medially, and the stomach is retracted to the right. The phrenicoesophageal ligament is transected circumferentially, the esophagus is released and pulled into the abdominal cavity, taking care to avoid damage of the ventricular branch of the vagus nerve. This manipulation leads to pneumothorax, and mechanical ventilation with positive pressure ventilation and thoracic evacuation are required. Phrenoplasty is performed for a distance of 1-2cm; the diaphragmatic crura are brought together ventrally of the esophagus with simple interrupted or horizontal mattress sutures using a monofilament non-absorbable suture. 11,14 At the end of the procedure, the surgeon must be able to insert one or two fingers into the hiatus along the esophagus without causing stenosis.10 With this technique, the caudal esophageal sphincter is moved dorsally. Some surgeons consider that phrenoplasty can be performed with no incision of the phrenoesophageal ligament, placing horizontal mattress sutures ventrally and dorsally through the diaphragmatic crura. 22 Esophagopexy is accomplished with the use of a few simple interrupted sutures between the esophagus and diaphragm on the left, or by making two 3cm incisions to the level of muscularis of the esophagus and on the diaphragm and suturing the incisions together (Figure 9). Finally, a left fundic incisional gastropexy is performed to anchor the stomach to the body wall, or a gastrostomy tube is placed so that the forward displacement of the stomach is prohibited (Figure 10). Gastropexy in this position achieves an increase in the pressure of the caudal esophageal sphincter, thus preventing GER. 38 The prognosis after surgery is very good or excellent. 11,15,16,22
Surgical treatment of HH is indicated if conservative treatment, which lasts 30 days, fails in type II-IV hernias and in Shar-Pei dogs. 12,15,16,22,47 Previously, surgical treatment of HH aimed to strengthen the caudal esophageal sphincter, which was considered to have failure or achalasia, with the use of various fundoplication techniques. These techniques were characterized by a high complication rate, and were abandoned because the theory of achalasia was eliminated.6,10-12,16 Nowadays, the surgical treatment of choice is the anatomical restoration and stabilization of HH.11 This surgery guarantees the best results with the use of the simplest surgical techniques. The surgery aims at the reduction in the hiatus diameter (phrenoplasty), fixation of the esophagus to the diaphragmatic crus with esophagopexy, and fixation of the stomach to the left abdominal wall with gastropexy (Figure 8).11 In the case of aspiration pneumonia, appropriate antibiotherapy should be administered preoperatively. The hiatus is approached through a median laparotomy after the passage of an orogastric tube through the esophagus to allow easier identification of the esophagus and hiatus: the hepatic ligament is transected, the left liver lobes are retracted medially, and the stomach is retracted to the right. The phrenicoesophageal ligament is transected circumferentially, the esophagus is released and pulled into the abdominal cavity, taking care to avoid damage of the ventricular branch of the vagus nerve. This manipulation leads to pneumothorax, and mechanical ventilation with positive pressure ventilation and thoracic evacuation are required. Phrenoplasty is performed for a distance of 1-2cm; the diaphragmatic crura are brought together ventrally of the esophagus with simple interrupted or horizontal mattress sutures using a monofilament non-absorbable suture. 11,14 At the end of the procedure, the surgeon must be able to insert one or two fingers into the hiatus along the esophagus without causing stenosis.10 With this technique, the caudal esophageal sphincter is moved dorsally. Some surgeons consider that phrenoplasty can be performed with no incision of the phrenoesophageal ligament, placing horizontal mattress sutures ventrally and dorsally through the diaphragmatic crura. 22 Esophagopexy is accomplished with the use of a few simple interrupted sutures between the esophagus and diaphragm on the left, or by making two 3cm incisions to the level of muscularis of the esophagus and on the diaphragm and suturing the incisions together (Figure 9). Finally, a left fundic incisional gastropexy is performed to anchor the stomach to the body wall, or a gastrostomy tube is placed so that the forward displacement of the stomach is prohibited (Figure 10). Gastropexy in this position achieves an increase in the pressure of the caudal esophageal sphincter, thus preventing GER. 38 The prognosis after surgery is very good or excellent. 11,15,16,22
> References
1. Hunt JB. Hiatal hernia. In: Mechanisms of Disease in Small Animal Surgery. Bojrab MJ, Monnet E (eds). 3rd edn. Teton New Media: Jackson, 2010, pp. 138-141.
2. Bright R. Hiatal hernia. In: Small Animal Soft Tissue Surgery. Monnet E(ed). 1st edn.Wiley- Blackwell: Ames, 2013, pp. 321-327.
3. Sivacolundhu RK, Read RA, Marchevsky AM. Hiatal hernia controversies – a review of pathophysiology and treatment options. Aust Vet J 2002, 80: 48-53.
4. Gordon LC, Friend EA, Hamilton MH. Hemorrhagic pleural effusion secondary to an unusual type III hiatal hernia in a 4-year-old Great Dane. J Am Anim Hosp Assoc 2010, 46: 336-340.
5. Cornell K. Stomach. In: Veterinary Surgery Small Animals. Tobias KM, Johnston SA (eds). 1st edn. Elsevier Saunders: St Louis, 2012, pp. 1500-1512.
6. Gaskell CJ, Gibbs C, Pearson H. Sliding hiatus hernia with reflux oesophagitis in two dogs. J Small Anim Pract 1974, 15: 503-509.
7. Robotham GR. Congenital hiatal hernia in a cat. Feline Pract 1979, 9: 37-39.
8. Dhein CRM, Rawlings CA, Rosin E, Losonsky JM, Chambers JN. Esophageal hiatal hernia and eventration of the diaphragm with resultant gastroesophageal reflux. J Am Anim Hosp Assoc 1980, 16: 517-522.
9. Peterson SL. Esophageal hiatal hernia in a cat. J Am Vet Med Assoc 1983, 183: 325-326.
10. Ellison GW, Lewis DD, Phillips L, Tarvin GB. Esophageal hiatal hernia in small animals: literature review and a modified surgical technique. J Am Anim Hosp Assoc 1986, 23: 391-399.
11. Prymak C, Saunders HM, Washabau RJ. Hiatal hernia repair by restoration and stabilization of normal anatomy an evaluation in four dogs and one cat. Vet Surg 1989, 18: 386-391.
12. Bright RM, Sackman JE, DeNovo C, Toal C. Hiatal hernia in the dog and cat: a retrospective study of 16 cases. J Small Anim Pract 1990, 31: 244-250.
13. Waldron DR, Moon M, Leib MS, Barber D, Mays KA. Oesophageal hiatal hernia in two cats. J Small Anim Pract 1990, 31: 259-263.
14. White RN. A modified technique for surgical repair of oesophageal hiatal herniation in the dog. J Small Anim Pract 1993, 34: 599-603.
15. Callan MB, Washabau RJ, Saunders HM, Kerr L, Prymak C, Holt D. Congenital esophageal hiatal hernia in the Chinese Shar-Pei dog. J Vet Intern Med 1993, 7: 210-215.
16. Lorinson D, Bright RM. Long-term outcome of medical and surgical treatment of hiatal hernias in dogs and cats: 27 cases (1978-1996). J Am Vet Med Assoc 1998, 213: 381-384.
17. Pratschke KM, Hughes JML, Skelly C, Bellenger CR. Hiatal herniation as a complication of chronic diaphragmatic herniation. J Small Anim Pract 1998, 39: 33-38.
18. Hardie EM, Ramirez O, Clary EM, Kornegay JN, Correa MT, Feimster RA, Robertson ER. Abnormalities of the thoracic bellows: stress fractures of the ribs and hiatal hernia. J Vet Intern Med 1998, 12: 279-287.
19. Papazoglou LG, Patsikas M, Rallis T, Galatos A, Adamama-Moraitou K. Hiatal hernia with esophageal stricture in a cat. Feline Pract 2000, 28: 10-14.
20. Hunt GB, O’Brien C, Kolenc G, Malik R. Hiatal hernia in a puppy. Aust Vet J 2002, 80: 685-686.
21. Owen MC, Morris PJ, Bateman RS. Concurrent gastro-oesophageal intussusception, trichobezoar and hiatal hernia in a cat. N Z Vet J 2005, 53: 371-374.
22. Guiot LP, Lansdowne JL, Rouppert P, Stanley BJ. Hiatal hernia in the dog: a clinical report of four Chinese Shar Peis. J Am Anim Hosp Assoc 2008, 44: 335-341.
23. Keeley B, Puggioni A, Pratschke K. Congenital oesophageal hiatal hernia in a pug. Irish Vet J 2008, 61: 389-393.
24. DeSandre-Robinson DM, Madden SN, Walker JT. Nasopharyngeal stenosis with concurrent hiatal hernia and megaesophagus in an 8-year-old cat. J Feline Med Surg 2011, 13: 454-459.
25. Teunissen GHB, Happe RP, Van Toorenburg J, Wolvekamp WTHC. Esophageal hiatal hernia case report of a dog and a cheetah. Tijdschr Diergeneeskd 1978, 103: 742-749.
26. Miles KG, Pope ER, Jergens AE. Paraesophageal hiatal hernia and pyloric obstruction in a dog. J Am Vet Med Assoc 1988, 193: 1437-1439.
27. Kirkby KA, Bright RM, Owen HD. Paraoesophageal hiatal hernia and megaoesophagus in a three-week-old Alaskan malamute. J Small Anim Pract 2005, 46: 402-405.
28. Mitsuoka K, Tanaka R, Nagashima Y, Hoshi K, Matsumoto H, Yamane Y. Omental herniation through the esophageal hiatus in a cat. J Vet Med Sci 2002, 64: 1157-1159.
29. Williams JM. Hiatal hernia in a Shar-Pei. J Small Anim Pract 1990, 31: 251-254.
30. Auger JM, Riley SM. Combined hiatal and pleuroperitoneal hernia in a Shar-Pei. Can Vet J 1997, 38: 640-642.
31. Baig MA, Gemmill T, Hammond G, Patterson C, Ramsey IK. Budd-chiari-like syndrome caused by a congenital hiatal hernia in a Shar-Pei dog. Vet Rec 2006, 159: 322-323.
32. Rahal SC, Mamprim MJ, Muniz LMR, Teixeira CR. Type-4 esophageal hiatal hernia in a Chinese Shar-Pei dog. Vet Radiol Ultrasound 2003, 44: 646-647.
33. Bremner CG, Shorter RG, Ellis FH. Anatomy of feline esophagus with special reference to its muscular wall and phrenoesophageal membrane. J Surg Res 1970, 10: 327-331.
34. Botha GSM. A note on the comparative anatomy of the cardio-esophageal junction. Acta Anat (Basel) 1958, 34: 52-58.
35. Clark CG, Vane JR. The cardiac sphincter in the cat. Gut 1961, 2: 252-262.
36. Pratschke KM, Fitzpatrick E, Campion D, McAllister H, Bellenger CR. Topography of the gastro-oesophageal junction in the dog revisited: possible clinical implications. Res Vet Sci 2004, 76: 171-177.
37. Alsafy MAM, El-Gendy SAA. Gastroesophageal junction of Anatolian shepherd dog; a study by topographic anatomy, scanning electron and light microscopy. Vet Res Commun 2012, 36:63-69.
38. Pratschke KM, Bellenger CR, McAllister H, Campion D. Barrier pressure at the gastroesophageal junction in anesthetized dogs. Am J Vet Res 2001, 62: 1068-1072.
39. Han E. Diagnosis and management of reflux esophagitis. Clin Tech Small Anim Pract 2003, 18: 231- 238.
40. Stickle R, Sparschu G, Love N, Walshaw R. Radiographic evaluation of esophageal function in Chinese Shar Pei pups. J Am Vet Med Assoc 1992, 201: 81-84.
41. Poncet CM, Dupre GP, Freiche VG, Estrada MM, Poubanne YA, Bouvy BM. Prevalence of gastrointestinal tract lesions in 73 brachycephalic dogs with upper respiratory syndrome. J Small Anim Pract 2005, 46: 273- 279.
42. Poncet CM, Dupre GP, Freiche VG, Bouvy BM. Longterm results of upper respiratory syndrome surgery and gastrointestinal tract medical treatment in 51 brachycephalic dogs. J Small Anim Pract 2006, 47: 137- 142.
43. Barnie AG, Simpson JW, Corcoran BM. Gastrooesophageal reflux and hiatus hernia associated with laryngeal paralysis in a dog. J Small Anim Pract 1989, 30: 414-416.
44. Dvir E, Spotswood TC, Lambrechts NE, Lobetti RG. Congenital narrowing of the intrapharyngeal opening in a dog with concurrent oesophageal hiatal hernia. J Small Anim Pract 2003, 44: 359-362.
45. Dieringer TM, Wolf AM. Esophageal hiatal hernia and megaesophagus complicating tetanus in two dogs. J Am Vet Med Assoc 1991, 199: 87-89.
46. Van Ham L, Van Bree H. Conservative treatment of tetanus associated with hiatus hernia and gastrooesophageal reflux. J Small Anim Pract 1992, 33: 289- 294.
47. Holt D, Callan MB, Washabau RJ, Saunders MH. Medical treatment versus surgery for hiatal hernias. J Am Vet Med Assoc 1998, 213: 800.
